Jay Lieberman
Jay Lieberman
DPM, FACFAS,
Director of
Podiatric Medical Education,
Northwest Medical Center |
 D. VonDerLinden
D. VonDerLinden
DPM,
Resident
Foot and Ankle Surgery,
Northwest Medical Center |
|
|
Case Study: Staged Limb Preservation with Integra Bilayer Matrix Wound Dressing
A 67 year old man presented to the Emergency Department complaining of painful bleeding ulcers to his bilateral lower extremities, the left being much worse than the right. Patient claimed the wounds had been present for greater than one year, beginning as a small wound with an insidious onset and later coalescing to form larger wounds. There was no precipitating trauma. He had received multiple treatment modalities with two different wound care doctors at different institutions. |
|
Treatment included weekly debridements, compression dressings and steroid creams. Antibiotic treatment included cultures revealing a heavy growth of Pseudomonas. The patient was maintained on Ciprofloxacin 750 mg twice daily. Wound biopsies came back negative for vasculitis and carcinoma.
The patient’s medical history was significant for acute atrial fibrillation with subsequent cardiac catheterization, temporal arteritis, prostate cancer, hypertension, hypothyroidism, pituitary adenoma, gastroesophageal reflux disease, chronic kidney disease, depression and anxiety. Patient was taking Percocet and a Fentanyl Patch for the pain to his lower extremities. Other medications include Zoloft, Aspirin, Metoprolol, Valium, Synthroid, Prednisone (for temporal arteritis), and Prevacid. Patient’s surgical history included prostectomy, right rotator cuff repair, right inguinal hernia repair and pituitary tumor resection. He denied tobacco or illicit drug use or alcohol intake.
Lower extremity physical examination revealed extensive full-thickness ulcerations to bilateral lower extremities, with the left being worse than the right. The wound was nearly circumferential at the left ankle (Figure 1). Bilaterally, the wounds demonstrated irregular borders, malodor, greenish purulence and severe sanguinous drainage which eventually ceased in the ED. The wound bases were mostly fibrotic and necrotic. The left Achilles tendon was exposed and devitalized. The extensor compartment and vital structures were visualized in the depth of the wound. Capillary refill time was less than 5 seconds bilaterally. There was +2 pitting edema. Pulses were non-palpable secondary to pedal edema. The periwound was erythematous. Protective threshold was diminished. Patient was able to elevate both legs and actively and passively dorsiflex and plantarflex both ankles albeit with pain.
Patient’s laboratory data revealed a white count of 17.4 k/mcL, hemoglobin of 9.5 g/dL, hematocrit of 28.5%, platelet count of 447,000, sodium of 120 mmol/L, potassium of 5.5 mmol/L, glucose of 114 mg/dL, BUN of 99 mg/dL and creatinine of 3.7 mg/dL. Bilateral arterial ultrasound showed biphasic flow above the knees. However, due to the extensive ulcerations, the study was limited distal to the popliteals. Radiographs of bilateral tibia and fibula showed signs of osteopenia, but no evidence of osteomyelitis, fracture, or gas. Cultures of both lower extremities were obtained, which revealed abundant growth of Pseudomonas aeruginosa. This was sensitive to both quinolones and flouroquinolones. Initial wound care consisted of moistened Aquacel AG, 4x4’s and kerlix. Patient was admitted for medical management and intravenous antibiotic therapy with pending Cardiology, Infectious Disease, Dermatology and Nephrology consults.
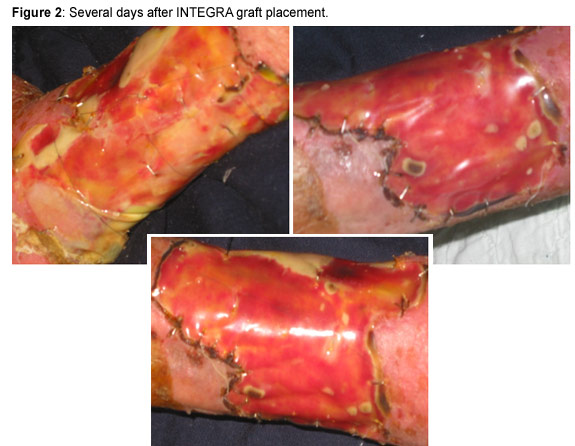
Patient began receiving Levaquin antibiotic therapy to treat the abundant Pseudomonas infection. A dermatology consult was ordered and dressing changes were modified to include topical corticosteroid (triamcinolone 0.1%) to the periwound daily. Seven days following admission, and after a full work up and subsequent medical clearance, the patient underwent surgical debridement with synthetic graft placement to left leg wounds (the right leg wounds were healing with local wound care). The initial goal of surgery was to remove the devitalized tissue, preserve the vital tissue and develop a granular base. The site was extensively debrided free of necrotic and fibrotic tissue, including a portion of the Achilles tendon. The graft utilized was the INTEGRA Bilayer Matrix Wound Dressing. This graft comprised a porous matrix of cross-linked bovine tendon collagen and glycosaminoglycan and a semi-permeable polysiloxane (silicone layer). The collagen-glycosaminoglycan biodegradable matrix provided a scaffold for cellular invasion and capillary growth while the semi-permeable silicone membrane controlled water vapor loss and increased tear strength. The operation and post-operative course was without incident. The first post operative dressing change showed acceptance of graft with normal phase incorporation (Figure 2). Patient was later discharged to a nearby rehabilitation center where he received continued local wound care.
While the patient’s wound to the left leg significantly improved as a result of the INTEGRA graft, further and aggressive care was still indicated (Figure 3). Repeat cultures grew out quinolone resistant Pseudomonas. Patient was then treated with meropenem. After discharge from the rehabilitation center, the patient was sent to another wound care center where the primary surgeon (plastic surgeon) was hopeful the patient would receive hyperbaric oxygen therapy. Unfortunately, the patient did not meet the qualifications for this treatment modality.
Patient received continued outpatient wound care treatment consisting of acetic acid washes with VAC therapy. Three and a half months following the initial graft placement, the patient was again brought to the OR where he underwent surgical debridement of left leg wound with xenograft placement (Figure 4). The goal here was to further proliferate the granular base.
Patient continued the VAC therapy for 10 days. After which, he was again brought to the OR for a third time, this time to receive a split thickness skin graft from the ipsilateral thigh (Figure 5).
The post operative course was without incident and the split-thickness skin graft was accepted and incorporated. After extensive and timely wound care management including, multiple debridements and graft placements, patient’s wounds have finally resolved (Figure 6). He maintains use of an AFO splint to the left lower extremity due to loss of the Achilles tendon.
As is well known, the practice of wound care requires tireless patience and the use of a wide range of treatment modalities. This patient, a 67 year old man, acquired small idiopathic wounds to his lower extremities which coalesced to extensive, deep, necrotic circumferential wounds. Various diagnoses have been posed for the cause of this patient’s extensive ulcerations: pyoderma gangrenosum, resistant bacterial infection, immunosuppressed state. Patient began a high dosage steroid therapy for his temporal arteritis several months prior to the wound development. Perhaps any minor insult to the lower extremity skin was not manageable in the immunosuppressed state. Other treating physicians reported pathergy, therefore, Pyoderma Gangrenosum was considered. However, this was never confirmed. This patient’s condition had only been complicated by the development of a resistant bacterial infection. However, the patient later showed improvement with various surgical debridements and graft placements. Ultimately, this patient required continued and aggressive wound care treatment despite his definitive diagnosis.
###
Gait & Foot Function Analysis Seminar
May 9-10 Seattle, WA • November 7-8 Orlando, FL
This seminar is a must for anyone who assesses foot function and gait abnormalities on a regular basis. Learn how in-shoe pressure mapping technology is used to analyze foot function and gait. You will gain an overall understanding of how to utilize pressure mapping technology to achieve treatment success. |
|
|
Visit www.tekscan.com/medical/webinars.html to learn more about our educational webinars and online training sessions!
To register for any of these events or for more information, please contact Christina Novak at 617-464-4500 x344 or [email protected].
The cost to register for the Gait & Foot Function Analysis Seminar is $99, all other events are free of charge. Space is limited for all events, so reserve your spot today! |
|
|